Body: A highly sensitized 60-year-old woman with end-stage renal disease due to biopsy-confirmed IgA nephropathy (IgAN) was referred to the National Kidney Registry (NKR) for paired kidney exchange along with her HLA-incompatible daughter. A proposed match through NKR showed excellent clinical and immunologic compatibility with no detectable DSA by SAB assay. However, the final T and B cell FCXM was unexpectedly positive, prompting chain termination. Because chain breaks in NKR carry a significant negative impact, a detailed investigation was undertaken: 1)Detailed patient’s history review 2)Reevaluate HLA antibody profile and strength using new serum samples 3)Treated the serum to identify and eliminate interferences: EDTA (routine), DTT, autologous cell adsorption, and adsorption with donor cells that have cross-reactive group HLA antigens 4)Performed surrogate FCXMs using treated samples against random donor cells with known HLA profiles.
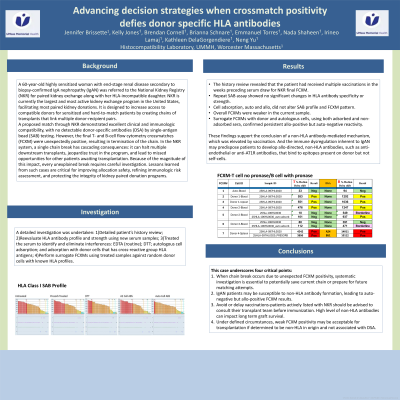
Results: The patient received multiple vaccinations in the weeks preceding the serum draw for NKR final FCXM. Repeat SAB assay showed no significant changes in HLA antibody specificity or strength. Cell adsorption, auto and allo, did not alter the SAB profile and FCXM pattern. Overall, FCXMs were weaker in the current sample. Surrogate FCXMs with donor and autologous cells, using both adsorbed and non-adsorbed sera, confirmed persistent allo-positive but auto-negative reactivity. These findings support the conclusion of a non-HLA antibody-mediated mechanism that was elevated by vaccination. The immune dysregulation inherent to IgAN may predispose patients to develop allo-directed, non-HLA antibodies, such as anti-endothelial or anti-AT1R antibodies, that bind to epitopes present on donor but not self-cells.
Conclusions: This case underscores four critical points: (1) When chain break occurs due to unexpected FCXM positivity, systematic investigation is essential to prepare for future matching attempts; (2) IgAN patients may be susceptible to non-HLA antibody formation, leading to auto-negative but allo-positive FCXM results; (3) avoid or delay vaccinations-patients actively listed with NKR should be advised to consult their transplant team before immunization; and (4) under defined circumstances, weak FCXM positivity may be acceptable for transplantation if determined to be non-HLA in origin and not associated with DSA.