– President/Laboratory Director, Texas Medical Specialty, Inc., United States
Body:
Introduction: Accurate HLA antibody interpretation is critical for donor eligibility and post-transplant monitoring. However, clinical laboratories have encountered challenges in selecting clinically appropriate HLA antibodies detection and MFI values. In our study, five heart and renal transplant recipients were successfully transplanted despite positive virtual, but negative physical crossmatches. The patients have been doing well for up to four years following transplantation. Donor specific antibodies (DSA) were investigated for binding to the cells by adsorption with cells bearing the relevant DSA antigens. None of the detected DSA bound to the cells and therefore were biologically irrelevant.
Methods: HLA typing were performed by Next Generation Sequencing. HLA antibody identification employed single antigen beads (SAB) and C1q assays. Patients’ sera were adsorbed with lymphocytes from surrogate donors bearing pertinent DSA antigens. AT1R was detected by ELISA assay.
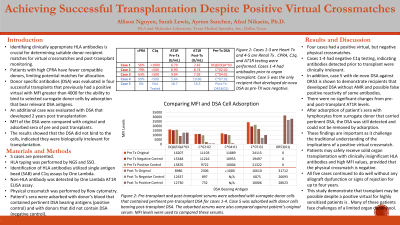
Results: Three heart transplant recipients had either DSA to HLA-C*02:02 (MFI=11,103), HLA-C*04:01 (MFI=11,889) or DQB1*03:02/DQA1*03 (MFI=16,207) of their potential donors. One renal transplant patient had DSA against HLA-C*07:02 (MFI=24,115) and the other against HLA-A*02:01 (MFI=1,695). All five patients had positive virtual, but negative physical crossmatches. Furthermore, all DSA were negative by C1q assay. Only one renal transplant recipient with DSA against HLA-C*07:02 received pre-operative IVIG and plasmapheresis to prevent unexpected complications. One of the heart transplant recipients with DSA had elevated AT1R and developed suspected rejection indicated by lower heart function which recovered quickly with treatment. DSA were still present at almost the same MFI values following adsorption with donors bearing pertinent DSA antigens which paralleled and supported the negative physical crossmatches. All patients continued to do well with no signs of rejection.
Conclusion: As demonstrated for the first time, not all antibodies detected by SAB are biologically relevant. Therefore, patients with pre-transplant existing DSA to selective HLA antigens may be safely transplanted. These findings are critical for accurate identification of HLA antibodies which may affect allocation of organs to highly sensitized patients or those who need immediate transplants.

.jpg "Afzal Nikaein, PhD, HCLD, ACHI (she/her/hers) photo")