– Associate Professor of Pathology, UC San Diego Health
Aim :To evaluate the utility of molecular ABO typing in deceased solid organ donors compared to serologic ABO typing.
Methods: Data was collected retrospectively on all molecular ABO typing performed on deceased donors between July 2023 through March 2025 (N = 42). Molecular ABO typing was performed on blood or buccal swab samples using LinkSeq ABO kit (Thermo Fisher). Molecular typing results were compared to serologic typing results uploaded into UNET for all donors. Data was also collected on number of transfusions received by each donor.
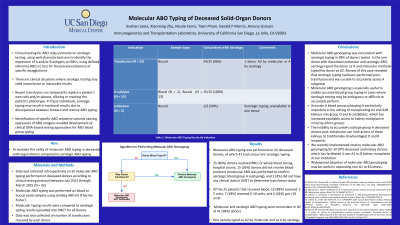
Results: Molecular ABO typing was performed on 42 deceased donors, of which 41 had concurrent serologic typing. Molecular and serologic ABO typing were concordant in 40 of 41 (98%) donors. Indication Sample type Concordant Comments
Transfusion (N = 25) Buccal 24/25 (96%) 1 donor A2 by molecular vs A by serology
Unknown (N = 2) Buccal 1/2 (50%) Serologic typing unavailable in one donor
Of the 25 patients that received blood, 12 (48%) received 1-5 units, 7 (28%) received 6-10 units, and 6 (24%) got >10 units.
Conclusion: There is growing evidence for the utility of molecular ABO genotyping in the setting of solid organ transplantation. Molecular ABO genotyping was concordant with serologic typing in 98% of donors tested. In the one donor with discordant molecular and serologic ABO, serology typed the donor as A and molecular methods typed the donor as A2. Review of this case revealed that serologic typing had been performed post-transfusion and was unable to accurately assess A subgroup. This highlights the utility of molecular ABO genotyping to enable accurate blood group typing in cases where serologic testing may be ambiguous or difficult to accurately perform.
Accurate A blood group subtyping is particularly important in the setting of transplanting A2 and A2B kidneys into group O and B candidates, which has increased equitable access to kidney transplant in minority ethnic groups. The inability to accurately subtype a group A deceased donor post-transfusion can limit access of these kidneys to traditionally disadvantaged O and B recipients. We recently implemented routine molecular ABO genotyping for all OPO deceased and kidney donors, which has facilitated 3 non-A1 to B kidney transplants at our institution. Widespread adoption of molecular ABO genotyping may be useful in expanding non-A1 to B kidney transplants.