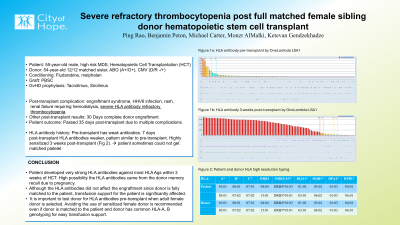
Body: A 55-year-old male with high risk MDS was evaluated for Hematopoietic Cell Transplantation (HCT). Patient was conditioning with Fludarabine and Melphalan (FM) and received PBSC graft followed by Tacrolimus and Sirolimus (T/S) for GvHD prophylaxis. Donor was 54 years old sister who was 12/12 HLA matched with major ABO mismatch (A+/O+) and CMV mismatch (D/R -/+). Patient’s post-transplant course was complicated with engraftment syndrome, HHV6 infection, rash, and renal failure requiring hemodialysis. Day 30 post HCT, peripheral blood chimerism test showed complete donor engraftment. However, patient developed severe HLA antibody refractory thrombocytopenia and needed transfusion support almost daily post-transplant during in-patient care. Patient passed 35 days post-transplant due to multiple complications. Patient’s HLA antibody history was the following: patient had weak HLA antibody reactivities against HLA-B57, B58, B49, B50 and A66:01(MFI 1050-3380, Fig1a) pre-transplant. No class II antibody was detected. One week post-transplant (before engraftment), HLA antibody profile was similar to pre-transplant with lower MFI ( < 791). Three weeks post-transplant (after engraftment), HLA antibody test was requested due to refractory thrombocytopenia. Class II antibody remained negative, however patient became broadly and strongly sensitized with 98% cPRA for class I and 2/3 beads with MFI > 10k(Fig1b). Given the breadth, strength and timing of HLA antibody development, we thought there is high possibility the HLA antibodies came from the donor memory recall. Since we did not routinely test donor HLA antibody pre-transplant and no donor serum was stored, we could not confirm our hypothesis and rule out other source of sensitization or passive transfer of antibodies. Regardless of patient’s common HLA-A, B typing (Fig2), there are several occasions matched platelet was not available which weaken patient support.
Conclusion: In HCT, we rarely test donor antibody profile, especially when the donor is a full match to the patient, as was the case here. This case reminds us the importance to test donor for HLA antibodies pre-transplant especially with adult female donor. Avoiding the use of a highly sensitized female donor is suggested even if the donor is a full match to the patient and donor has common HLA-A, B genotyping for easy transfusion support.