– Director, Technical Supervisor & Clinical Consultant , American National Red Cross, United States
Body:
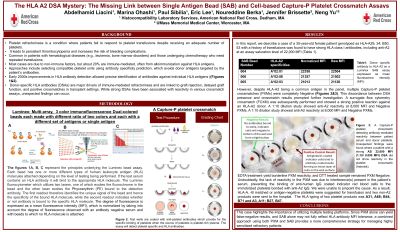
Background: Platelet refractoriness refers to a clinical condition in which a patient does not respond to platelet transfusions despite receiving an adequate number of platelets. This lack of response can result in persistent thrombocytopenia and an increased risk of bleeding. Platelet refractoriness can occur due to various underlying causes, and it is a significant concern in patients who require frequent platelet transfusions, such as those with leukemia, bone marrow disorders, or those undergoing chemotherapy. Donor-specific HLA antibody (DSA) is a common immune cause. While strong DSAs have been associated with reactivity in various crossmatch assays, unexpected findings can occur. In this report, we describe a case of a 35-year-old female patient genotyped as HLA-A29, 34; B50, 53 with a history of transfusions was found to have strong HLA class I antibodies, including anti-A2 at an assay saturation level of 22,000 MFI (Table 1). However, despite HLA- A2 being a common antigen in the panel, multiple Capture-P platelet crossmatches (PXMs) were completely Negative (Figure 1). This discordance between DSA presence and crossmatch results prompted further investigation. A surrogate flow cytometry crossmatch (FCXM) was subsequently performed and showed a strong positive reaction against an HLA A2 donor. A 1:10 dilution study showed anti-A2 reactivity at 8,000 MFI and Negative PXMs. EDTA treatment yield borderline PXM reactivity, and DTT treated sample remained PXM Negative. Undoubtedly, the lack of reactivity in the PXM was due to interference(s) present in the patient’s serum, preventing the binding of anti-human IgG coated indicator red blood cells to the immobilized platelets bonded with anti-A2 IgG. We were unable to pinpoint the cause. As a result, HLA-A, -B matched or antigen-negative platelets were suggested for transfusion and two non-A2 products were sent to the hospital. The HLA typing of two platelet products was A31, A68; B44, B71 and A3, A11; B27, B47.
Conclusion: This case highlights the importance of utilizing multiple testing platforms. Since PXM alone can yield false-negative results, and SAB alone may not fully reflect HLA antibody MFI tolerance, a combined approach using both PXM and SAB provides a more comprehensive strategy for managing highly sensitized refractory patients.

.jpg "Abdelhamid Liacini, PhD F(ACHI) HCLD/CC(ABB) photo")