– Lab Director, Penn State Hershey Medical Center, United States
Aim: Pre-transplant donor-specific HLA antibody (DSA) increases risk of engraftment failure in allogenic stem cell transplant (SCT). After initial sensitization, HLA antibody may wax or wane, depending on the level of antigen exposure (ex. transfusion), disease-mediated inflammation, or chemoradiation-caused tissue injury. Impacts of gender and diagnosis on pre-transplant HLA antibody was evaluated.
Methods: HLA antibody prevalence (2016-2024) before first SCT was reviewed in patients with acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), acute lymphocytic leukemia (ALL), myelofibrosis (MF), aplastic anemia (AA), lymphoma, chronic myeloid leukemia (CML), and chronic myelomonocytic leukemia (CMML). HLA antibody was considered present when PRA >0% by Labscreen PRA using a cutoff of ≥1000 MFI (Thermofisher, CA). Prevalence of HLA antibody (% patient) was compared by the Fisher Exact Test (p < 0.05).
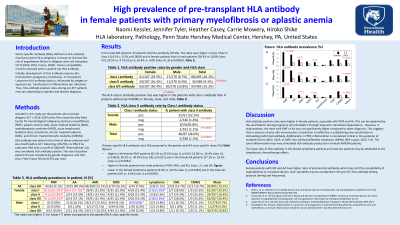
Results: HLA antibody was present in 92/485 patients (19.0%), which prevalence was higher for class I (87/485 patients, 17.9%) than for class II (45/485 patients, 9.3%), and in female (63/207 patients, 30.4%) than in male (29/278 patients, 10.4%). Female patients with MF and AA showed especially high HLA antibody class I/II prevalence (9/13 and 8/14 patients, 69.2% and 57.1%, respectively, Fig. A) than in AML (29/91 patients, 31.9%), MDS (8/35 patients, 22.9%), ALL (5/26 patients, 19.2%), lymphoma (7/17 patients, 5.6%). The higher prevalence is accounted by class I and II antibody in MF (8/13 and 7/13 patients, 53.8% and 61.5%, respectively, Fig. B/C) and class I antibody in AA (8/14 patients, 57.1%). In males, class I antibody showed lower prevalence in ALL (0/50 patients, 2.0%) than with the remaining diseases (26/228 patients, 11.4%). In males, class II antibody showed no significant difference in prevalence among diagnosis (11/278 patients, 4.0%).
Conclusion: Female patients with MF and AA have high prevalence of HLA antibody. This may be attributed to pregnancy, proinflammatory disease (MF), and transfusion dependency (AA). These patients are at high-risk of DSA when haploidentical or unrelated donors are selected. HLA antibody testing protocol (timing and frequency) may be optimized according to the risk.
Footnotes: Figure: HLA antibody prevalence (%patient) is shown among various hematological diseases for class I and II (A), class I only (B), and class II antibody only (C).

 photo")