(307) Virtual Crossmatch Compatible with Unexpected Fluorescence Cytometric Crossmatch Positive, may be Safe to Proceed with Transplantation under Certain Circumstances
– Medical Laboratory Scientist; Lead Technologist , UAMS
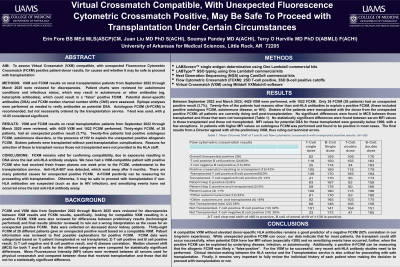
Aim: To assess Virtual Crossmatch (VXM) compatible with unexpected Fluorecence Cytometric Crossmatch (FCXM) positive results for causes and whether it may be safe to proceed with transplantation.
Methods: VXM and FCXM results on renal transplantation patients from September 2022 through March 2025, and records were reviewed for autoimmune condition and infectious status, which may result in autoimmune or other antibodies, which could result in a “false” positive FCXM. Potential donor-specific antibodies (DSA) and FCXM median channel number shifts (CNS) were assessed. Epitope analyses were performed as needed to verify antibodies. Autologous FCXM (A-FCXM) is recommended, but not necessarily ordered. T-test was used, with p <0.05 considered significant.
Results: 4500 VXM with 506 (11% of total) FCXM were performed. 38 (7.5% of FCXM) discrepancies (VXM compatible and FCXM positive) were found from 28 patients. 25 of the patients had potential causes, which were considered as reasons for having auto-reactive, non-HLA antibodies, which could result in a “false” positive FCXM: SLE (4, 16%), other autoimmune disease (12, 48%), HIV+ (1, 4%), HepB+ (1, 4%), CMV+ (4, 16%) and/or HepC+ (3, 12%). 16 (42% of the discrepant) patients proceeded to transplantation. (One each: HepC+, Malignant melanoma and CMV+, Jeune syndrome, Basal carcinoma [A-FCXM +], IgA nephropathy, HepC+ and HepB+, MS/FSGS, PLAR2 membranous nephropathy, Celiac disease, SLE, Platelet dysfunction associated with uremia, PCKD/Celiac disease, HIV+, no condition found [A-FCXM +], no condition found [A-FCXM +], no condition found). There are no statistically significant differences in the CNS for those transplanted versus those not transplanted. There are no statistically significant differences in DSA values between those transplanted versus those not transplanted. The decision not to proceed with transplantation was made by the transplantation service.
Conclusion: FCXM remains valid for confirming compatibility, due to exposures resulting in DSA since the last check. There are many potential causes for unexpected positive FCXM. A-FCXM positivity can be reassuring for proceeding with transplantation. Otherwise, it may be safe to proceed with transplantation if non-HLA antibodies are suspected, and sensitizing events have not occurred since the last anti-HLA antibody assay.