(305) Incremental Clinical Benefit (ICB) and Cost Effectiveness Ratio (ICER) of Routine Flow Cytometric Crossmatch (FCXM) Prior To Kidney Transplantation
Aim: We have shown that rigorous molecular diagnostic testing using Next-Generation Sequencing (NGS) and Single Antigen Bead (SAB) methods to avoid HLA pre-sensitization significantly reduces the incidence of AMR rate. Within this context, we examine the value of routine pre-transplant FCXM, often used to further inform selection and management. Methods Recipient-donor pairs transplanted from 2016-2023 without historical or current DSA by SAB (threshold 1,000 MFI or lower based on epitope analysis) were stratified according to their pre-transplant FCXM. Patients with a +ve FCXM were reviewed to confirm their negative SAB history and transplanted. All were managed using standard guidelines and followed throughout their course by a single specialist team. ICB was analyzed using Cox proportional hazards models with stepwise selection, and economic outcomes using ICER. Results Of the 1,857 patients transplanted (462 LD, 1395 DD), 68 (3.7 %) had a positive FCXM; 31 (1.67 %) T-cell, 46 (2.48 %) B-cell and 9 (0.05 %) both. During the 6 years of observation, 228 patients (12.3 %) developed biopsy-confirmed acute rejection (BCAR), 206 (11.1 %) lost their graft and 170 (9.1 %) died. Unadjusted (Figure 1, Kaplan-Meier) or adjusted (Cox analysis) survival analysis incorporating cardinal baseline variables did not show any significant influence of pre-transplant FCXM on BCAR (T-FCXM: p=0.87 B-FCXM: p=0.57), graft loss (T-FCXM: p=0.95; B-FCXM: p=0.75) or death (T-FCXM: p=0.47; B-FCXM: p=0.37). Assuming an incremental unit cost of approximately $100 / FCXM test / patient, and no observable improvement in clinical outcome, the ICER of routine FCXM approaches infinity.
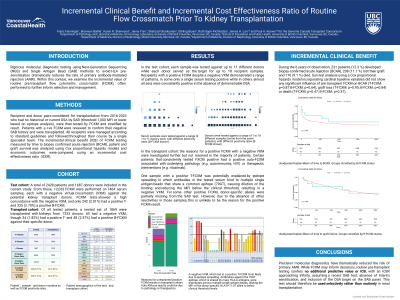
Conclusion: Precision molecular diagnostics have dramatically reduced the risk of primary AMR. While FCXM may inform decisions, routine pre-transplant testing confers no additional predictive value or discernable ICB, with an ICER approaching infinity. This test should therefore be used selectively rather than routinely in renal transplantation.